Real-World Impact
What these numbers mean for actual patient predictions
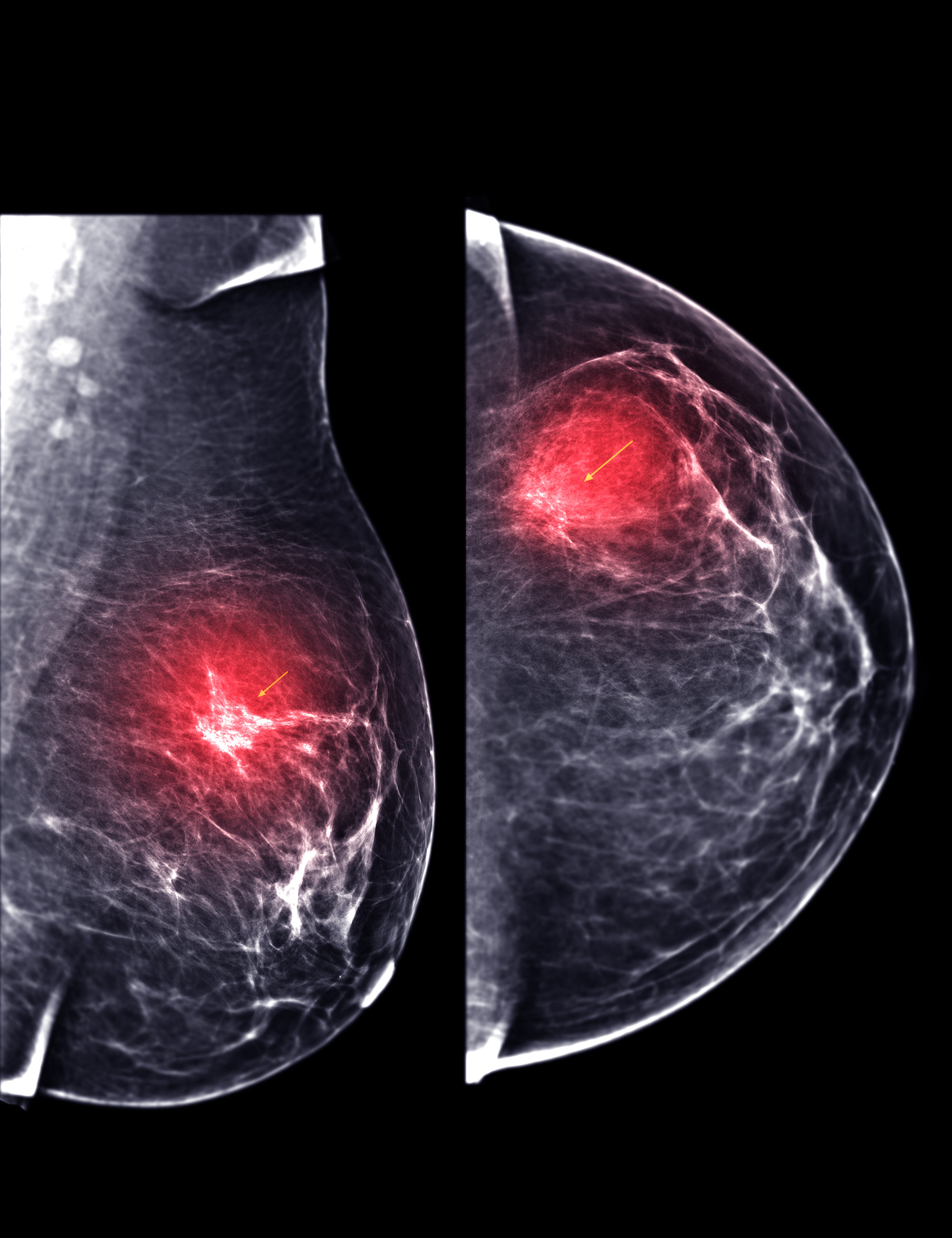
Mammography: Standard diagnostic imaging for breast cancer detection and monitoring
Study Dataset
4,024
patients
3,408
alive (84.7%)
616
dead (15.3%)
Clinical Impact: Without Progesterone Status, the model incorrectly predicts survival outcomes for an additional 246 breast cancer patients out of 4,024. That's roughly 6 extra wrong predictions for every 100 patients we assess.
Progesterone Status
✓ Critical to KeepWhen Kept
2,825
correct predictions
(70.2% accuracy)
(70.2% accuracy)
When Dropped
2,579
correct predictions
(64.1% accuracy)
(64.1% accuracy)
Impact When Dropped
246
additional patients
misclassified
misclassified
Clinical Impact: By excluding Regional Node Examined, the model correctly predicts outcomes for an additional 153 patients. That's about 4 more correct predictions per 100 patients. This feature adds noise because the model already includes "Regional Node Positive" which provides better signal.
Regional Node Examined
✗ Better to DropWhen Kept
2,797
correct predictions
(69.5% accuracy)
(69.5% accuracy)
When Dropped
2,950
correct predictions
(73.3% accuracy)
(73.3% accuracy)
Impact When Dropped
+153
additional patients
correctly classified
correctly classified